Posted in Asthma | 15/03/2015
The following drugs were used in the study: sterile solution of enprofylline 10 mg/ml and a matching sterile placebo solution (saline); the terbutaiine was in the form of Bricanyl 1 percent nebulizer solution together with a matching placebo nebulizer solution. The enprofylline was administered in a dose of 0.2 ml or 2 mg/kg, made up to 100 ml with normal saline solution at room temperature, via a burette, over 20 minutes. One ml (10 mg) of terbutaiine solution was made up to 3 ml with normal saline solution for administration via a Hudson nebulizer and a face mask using a flow rate of 6 L/min of oxygen for ten minutes. Patients were stratified for age (less than 45 years, and 45 years or more) and treatment allocation was randomized into blocks of four using a computer program. A double-blind technique was used so that each patient received simultaneously both an…
Read more

Posted in Asthma | 12/03/2015
The treatment of patients with acute asthma requires pharmacologic therapy with bronchodila-tors, corticosteroids, oxygen and other appropriate supportive measures. Inhaled betag agonists and intravenous xanthines are the most commonly used bronchodilator medications in acute asthma. Earlier studies in patients with acute asthma have usually compared the bronchodilating effects of inhaled selective betas agonists alone, and combined with intravenous xanthines in patients with acute asthma.
Read more
Posted in Pulmonary Function | 11/03/2015
Our results are close to those published by Thung et al. These authors found Vo2resp to be 13 percent of Vo2tot in patients studied after cardiac surgery. Higher values have been reported by Wilson et al in the immediate postoperative period of cardiac surgery. In patients with various degrees of cardiorespiratory diseases, Vo2 resp was found three times higher than that reported in the present study2 (8.7 vs 2.6 ml OJh of ventilation). This is related to the underlying lung disease which is associated with an increased work of breathing and/or a decreased efficiency of the respiratory muscles.
Read more
Posted in Airway | 09/03/2015
Although we performed these studies using only one ventilator manufacturers pressure-support system, we nevertheless believe that the principles we have discussed will apply to other available ventilator pressure-support systems as well; however, variability in factors such as the effectiveness in achieving and maintaining the set level of pressure support and the mechanism by which pressure support is terminated at the end of inspiration will affect the particular relationship between optimal pressure support and Vt/Ti as derived in this study. For instance, a ventilator circuit with higher resistance would require higher levels of pressure support at a given Vt/Ti and endotracheal tube diameter. Therefore, the specific regressions derived in this study for selecting the optimal level of pressure support may not apply to other ventilator systems.
Read more
Posted in Airway | 08/03/2015
Pressure-support ventilation has been suggested as a method by which to compensate for the increase in inspiratory work produced by endotracheal tubes and demand valve CPAP circuits; however, there has been no previous documentation which validates this proposed clinical application. Our findings indicate that pressure support may be useful for this purpose. We observed that as pressure support is increased, the added inspiratory Waw produced by the resistance of the endotracheal tube and demand valve circuit decreased. For each endotracheal tube, linear relationships between the pressure support needed to result in zero Waw and mean inspiratory flow were established.
Read more
Posted in Airway | 06/03/2015
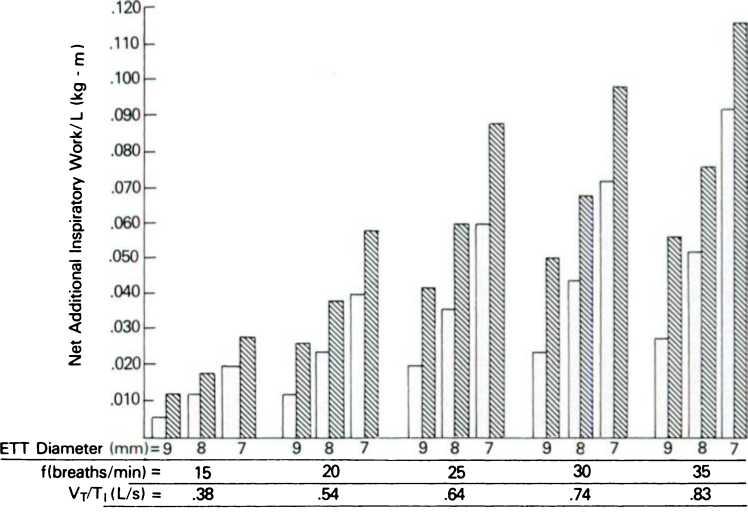
This study confirms that endotracheal tubes and a ventilator demand CPAP system can markedly increase the inspiratory work of breathing. The additional work rate (Wi/L) due to these added resistances increases with increased flow demand and decreased internal diameter of the tube. Pressure support can be used to compensate for this added work when the level is adjusted for the endotracheal tubes diameter and mean inspiratory flow. The effect of the endotracheal tubes size on airway resistance and work of breathing is substantial. Bolder and associates2 have reported that every 1-mm decrease in the endotracheal tube s diameter results in an increase in work of 34 to 154 percent, depending on the respiratory rate and tidal volume. In the mechanical-lung phase of this study, our findings were similar, with each 1-mm change in the tube s diameter resulting in a 67 to 100 percent increase in Wi/L. The effect of…
Read more
Posted in Airway | 05/03/2015
Mechanical Model The net added inspiratory work (Waw) increased progressively with decreasing size of the endotracheal tube and with increasing Vt/Ti (Fig 3). Each 1-mm decrease in the tubes diameter resulted in a 67 to 100 percent increase in work. Adding the ventilator circuit increased the work further. The proportion of added work due to the endotracheal tube alone, when compared to the added work for the tube and ventilator together, was a function of the tubes size. On average, a 9-mm tube contributed 50 percent of the total added work, with 8-mm and 7-mm tubes contributing 60 and 70 percent, respectively.
Read more