Granulomatous Pneumocystis carinii Pneumonia in Three Patients with the Acquired Immune Deficiency Syndrome: Case 2
 Case 2
Case 2
A 28-year-old woman with no known risk factors for AIDS was admitted to the Mount Sinai Hospital with a 9-kg weight loss, fever, shortness of breath, nonproductive cough, and oral thrush. Chest x-ray film showed slightly increased interstitial markings and a stellate nodular density in the right upper lobe (Fig 4). She underwent fiberoptic bronchoscopy, and transbronchial biopsies were obtained under fluoroscopic guidance. Routine histologic sections were prepared and stained with hematoxylin-eosin, Grocott methenamine silver, Ziehl Nielsen acid-fast, and Giemsa stains. An intra-alveolar and interstitial infiltrate of pale staining histiocytic-appearing cells and lymphocytes was seen. No multinucleated giant cells were present. There was also focal intra-alveolar foamy acellular eosinophilic exudate. Cysts of P carinii were readily found both within the areas of exudate as well as in the granulomatous areas. No other organisms were identified. The patient was treated with IV trimethoprim-sulfamethoxazole for three weeks and had clinical and radiologic improvement. Culture of transbronchially obtained material eventually grew Mycobacterium avium-intracellulare. HIV antibody tests were not performed.
Case 3
A 32-year-old Hispanic male IV drug abuser presented to the Bronx Veterans Administration Medical Center with a two-week history of shortness of breath and cough. Chest x-ray film revealed bilateral fluffy infiltrates. Transbronchial biopsies were processed for routine histologic sections and stained similarly to those in case 1. Histologically the case showed a picture nearly identical to that of case 2, except that the granulomas were better formed (Fig 5). Cysts of P carinii again were the only organisms identified (Fig 6), and cultures of the biopsied material were negative. The patient was treated with trimethoprim-sulfamethoxazole followd by pentamidine and showed clinical improvement. HIV antibody tests were not performed.
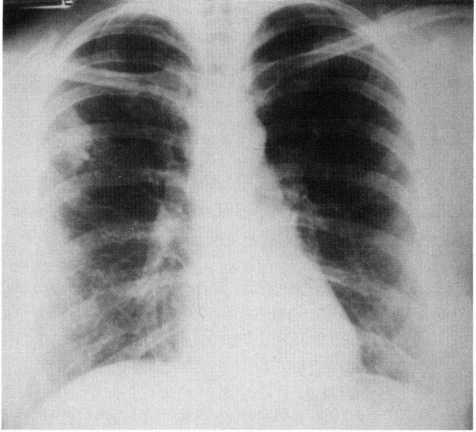
Figure 4. Chest x-ray film (case 2) showing ill-defined stellate density in right upper lobe and increased interstitial markings bilaterally.

Figure 5. Transbronchial biopsy specimen (case 3) showing a better formed granuloma composed of histiocytic cells and a few lymphocytes. (Hematoxylin-eosin X 200.)

Figure 6. Area identical to that in Figure 5 showing numerous cysts of Pneumocystis carinii within the granuloma (arrow). (Grocott methenamine silver x200.)
Category: AIDS
Tags: AIDS, biopsy, carinii pneumonia