A Classic Image of Complete Right Main Bronchus Avulsion
 A 26-year-old man was the front seat passenger in a car involved in a head-on collision. He was brought to the emergency room of a local hospital, where initial evaluation showed a mild dyspnea and a deep, 4-cm, left-sided cervical laceration through which air was heard gushing out. A roentgenogram of the chest revealed a right-sided tension pneumothorax. A chest tube was inserted into the right pleural space and the patient transferred. Upon arrival, some 6 h after the accident, the patient was conscious and neither dyspneic nor unstable. Minimal subcutaneous emphysema was present over the left side of the neck, and large air leaks from both the chest tube and the cervical wound were noted. There were no associated injuries.
A 26-year-old man was the front seat passenger in a car involved in a head-on collision. He was brought to the emergency room of a local hospital, where initial evaluation showed a mild dyspnea and a deep, 4-cm, left-sided cervical laceration through which air was heard gushing out. A roentgenogram of the chest revealed a right-sided tension pneumothorax. A chest tube was inserted into the right pleural space and the patient transferred. Upon arrival, some 6 h after the accident, the patient was conscious and neither dyspneic nor unstable. Minimal subcutaneous emphysema was present over the left side of the neck, and large air leaks from both the chest tube and the cervical wound were noted. There were no associated injuries.
The upright PA chest roentgenogram (Fig 1) showed a persistent tension pneumothorax on the right side with contralateral deviation of the heart and mediastinum. Because the superior border of the collapsed lung had fallen below the level of the right main stem bronchus, the image was interpreted as being characteristic of complete right main bronchus avulsion. Based on both the clinical picture and the radiologic findings, the patient was taken to the operating room for immediate surgical exploration and repair.
Diagnosis: Multiple lacerations of the intrathoracic and cervical trachea
Under topical anesthesia and while breathing spontaneously, the patient was first intubated with a single lumen tube. Flexible bronchoscopy done through the endotracheal tube showed a 5-cm longitudinal laceration of the membranous trachea above the carina (Fig 2A). A right posterolateral thoracotomy was then performed and the tracheal laceration easily repaired with interrupted absorbable sutures. The right main bronchus and pulmonary artery were noted to be intact, but the right lung remained atelectatic until the laceration was completely sutured. It then expanded easily.
Following closure of the thoracic incision, the patient was turned on his back and the cervical wound explored. A separate, transverse and stellate laceration of the cervical trachea (Fig 2b), which had not been seen at bronchoscopic examination, was identified and repaired. The esophagus, cervical blood vessels, and recurrent nerve were uninjured. Postoperative recovery was uneventful, and a chest roentgenogram obtained following repair (Fig 3) demonstrated complete reexpansion of the right lung.
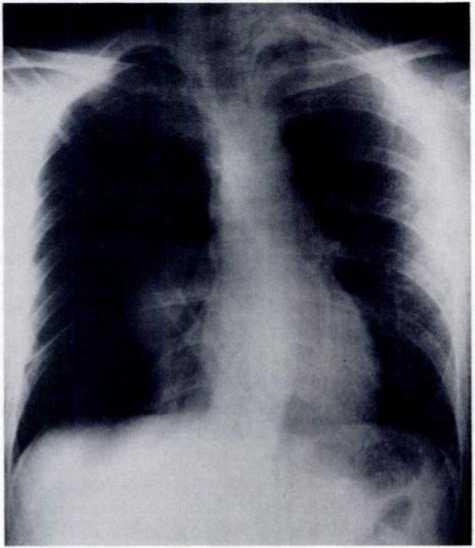
Figure 1
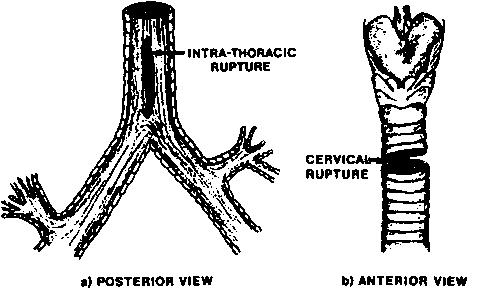
Figure 2

Figure 3
Category: Bronchus Avulsion
Tags: air-filled bronchus, bronchus avulsion, Pneumothorax