Ventricular Fibrillation Complicating Acute Myocardial Infarction: Materials and Methods
Selection of Patients
From the initial population studied, 35 were excluded because of the presence of other factors known to predispose or to be associated with ventricular arrhythmias. The criteria for exclusion that were applied (developed prior to the examination of the patients data) were as follows: (a) patients treated with group 1 antiarrhythmic drugs, digoxin, amiodarone, or sympathomimetic drugs prior to the onset of VF, with or without prolonged Q-Tc interval; (b) patients with previously known ischemic cardiomyopathy, ventricular arrhythmias, congestive heart Mure, or left ventricular aneurysm; (c) patients with serum potassium concentration of less than 3.5 mmol/L or more than 5.5 mmol/L (samples of blood were taken on admission); (d) patients with severe hypotension or cardiogenic shock; (3) patients with catheter-induced VF; and (f) patients in whom stages of AMI could not be recognized (complete left bundle-branch block, etc).
The remaining 34 patients who fulfilled the criteria for entry into the study were divided to two groups: (1) group 1 consisted of seven patients with fast disorganized ventricular activity, small voltage (<10 mm), an irregular, nonunifbrm undulated tracing, and no clear identifiable QRS complex (fine VF) (Fig 1); and (2) group 2 consisted of 27 patients with fast ventricular activity (>300/min), multiform QRS configuration with marked changes in the amplitude, and twisting axis (polymorphous or coarse VF) (Fig 2). Rhythm strips of VF were analyzed by two observers at an identical time three seconds from the beginning of VF. cheap-asthma-inhalers.com
Statistical Analysis
All data are presented as the mean ± standard deviation. The Fischer test was used in order to find statistical differences between the two groups. A level less than 0.05 was considered statistically significant.
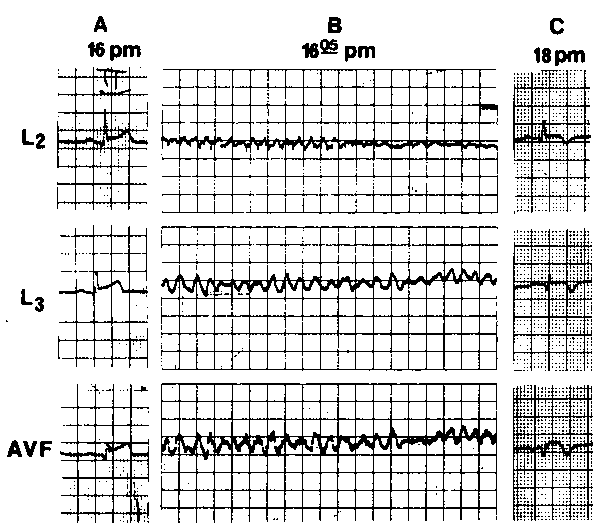
Figure 1. Example of type 1 VF in patient with inferior wall infarction (patient 1; Table 1). A. Electrocardiogram on admission (leads 2, 3, and aVF), demonstrating stage 1 of inferior wall infarction with minimal Q waves (<2 mm). B. Type 1 VF (fine VF). C. Two hours later. Stage 3 of inferior wall infarction is observed.
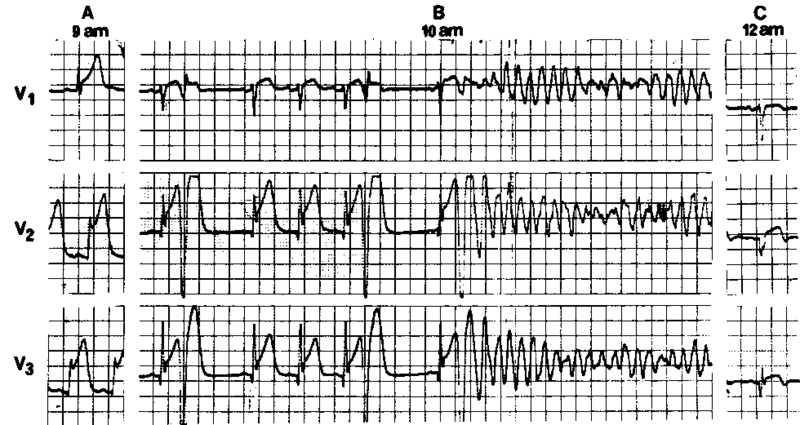
Figure 2. Three-channel ECG showing evolution of anterior wall myocardial infarction complicated by type 2 VF (patient 21; Table 3). A. Electrocardiogram on admission (leads V^ V2, and V3), showing stage 1 of anterior wall infarction. B. Type 2 VF (polymorphous VF) during stage 2 of AMI (Q waves more than 2 mm are seen before onset of VF). C. Two hours later. Stage 3 of anterior wall infarction is observed.
Table 1—Clinical and Electrocardiographic Data on Seven Patients with Type 1 VF Complicating AMI
| Patient, Sex, Age (yr) | CardiacRisk
Factors* |
PreviousCardiac
Diseaset |
Phaseof
AMI |
Localization of AMI* | Onset of VF, hours after admission} | No. of Episodes | Total No. of DC Shocks | Complications!! |
| 1,M,79 | AP | 1 | IW | OA | 1 | 1 | SVT; reinfarction | |
| 2,M,53 | AP; MI | I | IN/LA | 1.5 | 1 | 1 | SVT | |
| 3,M,58 | AH | MI | 1 | EX/AN | OA | 3 | 3 | |
| 4,M,39 | Smoking | 1 | EX/AN | OA | 1 | 1 | ||
| 5,M,50 | Smoking | AP | 1 | ASW | OA | 1 | 1 | |
| 6,M,66 | AH | 1 | EX/AN | OA | 1 | 1 | CS; death | |
| 7,M,58 | Smoking | AP | 2 | EX/PO | 16 | 1 | 1 | VF (type 2) |
Category: Myocardial Infarction
Tags: electrocardiographic, myocardial infarction, ventricular fibrillation